

On this page:
2.1 Biological Reductionism 2.2 Brain Imaging Techniques 2.3 Chemical Messengers 2.4 Diathesis-Stress Model 2.5 Social Learning Theory in Health and Wellbeing Practice QuestionsBiological reductionism is the approach of explaining complex psychological phenomena — including thoughts, emotions, behaviours, and mental disorders — by reducing them to their most basic biological components, such as neurons, neurotransmitters, hormones, and brain structures. The underlying assumption is that if we fully understand the biological machinery of the brain and body, we can explain all of psychology.
Biological reductionism takes many forms in psychology. The serotonin hypothesis of depression is one of the most well-known examples: this hypothesis proposes that depression results from insufficient serotonergic activity in the brain. This reductionist explanation led directly to the development of Selective Serotonin Reuptake Inhibitors (SSRIs) such as fluoxetine (Prozac), which increase serotonin availability in synaptic gaps by blocking its reuptake. Because SSRIs helped many people with depression, this seemed to confirm the biological model.
Similarly, aggression has been explained in reductionist terms through testosterone — higher testosterone levels in males have been associated with increased aggression, though the relationship is correlational rather than clearly causal. Anxiety disorders have been linked to overactivity in the amygdala. ADHD has been framed as a dopamine dysregulation disorder.
Brain imaging techniques allow researchers and clinicians to observe the structure and activity of the living human brain without surgery. These tools have transformed biological psychology by making it possible to study the neural correlates of behaviour, emotion, and cognition directly. The two most commonly used imaging techniques in psychology are functional magnetic resonance imaging (fMRI) and positron emission tomography (PET).
fMRI measures brain activity indirectly by detecting changes in blood oxygenation. The technique is based on the BOLD signal (Blood-Oxygen-Level-Dependent): when a brain region becomes active, it requires more oxygen, which increases blood flow to that area. fMRI detects the difference in magnetic properties between oxygenated and deoxygenated haemoglobin and maps these differences onto brain anatomy with high spatial resolution.
fMRI does not require injections or radiation, making it relatively safe and suitable for repeated use. Participants can perform tasks inside the scanner, allowing researchers to observe which brain regions activate during specific cognitive or emotional activities. For example, Raine et al. (1997) used PET scans to compare the brain activity of murderers who pled not guilty by reason of insanity against matched controls. They found reduced activity in the prefrontal cortex — a region involved in impulse control and decision-making — and abnormal activity in areas linked to emotion regulation. This provided biological evidence that violent behaviour may be associated with specific neurological differences.
PET scanning involves injecting a participant with a radioactive tracer that binds to specific molecules such as glucose or neurotransmitter receptors. As the tracer decays, it emits positrons that produce detectable gamma rays, allowing the scanner to map which brain areas are most metabolically active. PET has lower spatial resolution than fMRI but can measure specific neurotransmitter activity, making it particularly useful for studying dopamine and serotonin systems in addiction and mood disorders.
Applications and Evaluation
Brain imaging has provided valuable insights into the neural basis of mental disorders. Studies using fMRI have shown hippocampal volume reduction in individuals with PTSD, amygdala hyperactivity in social anxiety disorder, and altered prefrontal connectivity in depression. These findings have supported biological models of mental illness and guided pharmacological treatment development.
However, brain imaging techniques have important limitations. fMRI data is correlational — activation in a brain region during a task does not prove that region causes the behaviour. The statistical thresholds used to identify significant activation have been a source of controversy, with some studies found to report false positives. Reverse inference — concluding that a mental state caused an observed pattern of brain activation — is logically problematic because most brain regions participate in many different processes. Additionally, imaging studies often use small samples that are not representative of broader populations.
Chemical messengers are biological molecules that transmit signals within and between cells. In psychology, the most relevant chemical messengers are neurotransmitters, which carry signals between neurons across synaptic gaps, and hormones, which are released into the bloodstream and affect distant organs and tissues. Both systems regulate a wide range of physiological and psychological states.
Neurotransmitters are released from presynaptic terminals and bind to receptors on the postsynaptic neuron, either exciting or inhibiting it. Key neurotransmitters include:
Hormones are released by glands of the endocrine system and travel through the bloodstream to target organs. Cortisol, released by the adrenal cortex in response to stress, is closely studied in health psychology. While short-term cortisol elevation aids the stress response by mobilising energy, chronic cortisol elevation has damaging effects on the hippocampus, immune system, and cardiovascular health. Testosterone, estrogen, and oxytocin are also studied for their roles in aggression, social bonding, and mood.
Evaluation
Understanding chemical messengers has produced effective treatments and valuable insights into the biological substrates of behaviour. However, chemical messenger systems are highly complex and interactive. A simple model of 'too much' or 'too little' of any single neurotransmitter rarely captures the full picture. Serotonin affects dozens of receptor subtypes across multiple brain systems, meaning that manipulating it pharmacologically has wide-ranging effects. Reductionist explanations focused on single chemicals risk obscuring the importance of neural circuits, environmental context, and individual variation.
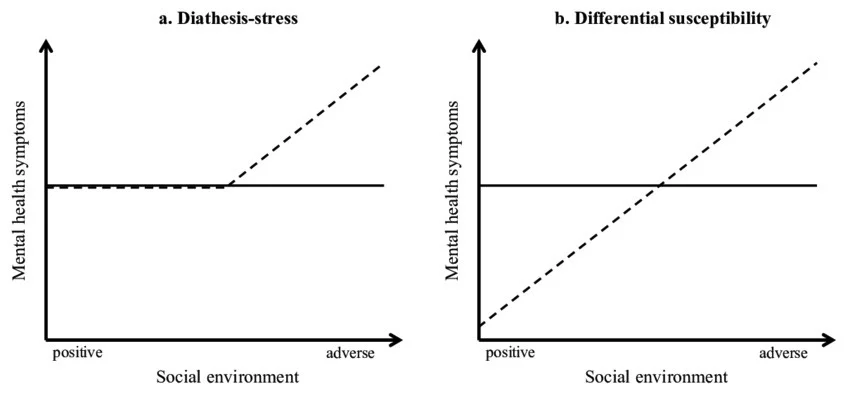
The diathesis-stress model is a framework for understanding how psychological disorders develop. It proposes that a disorder emerges from the interaction between a predispositional vulnerability (the diathesis) and environmental stress. The diathesis alone is not sufficient to produce a disorder; similarly, stress alone does not cause disorder in people without the relevant vulnerability. It is the combination of the two that produces illness.
Diathesis: a pre-existing vulnerability that makes an individual more susceptible to developing a disorder. Diatheses may be genetic (carrying a variant of the 5-HTT gene), biological (an overreactive amygdala), or psychological (a ruminative cognitive style or low self-esteem).
Stress: environmental triggers — life events or chronic conditions that place demands on the individual's coping resources. Stressors can include bereavement, relationship breakdown, trauma, financial hardship, childhood adversity, or major life changes.
Caspi et al. (2003) conducted a longitudinal study examining the interaction between the 5-HTT gene (short allele variant associated with lower serotonin transporter activity) and stressful life events in predicting depression. They followed over 1,000 New Zealand participants from birth to age 26. Participants who had the short allele of the 5-HTT gene and experienced multiple stressful life events were significantly more likely to develop depression than those with the long allele, or those with the short allele but low stress. This study is considered strong evidence for the gene-environment interaction at the heart of the diathesis-stress model.
Evaluation: The diathesis-stress model is valuable because it transcends the nature-nurture dichotomy, recognising that biology and environment work together. It helps explain why individuals with the same genetic makeup (such as identical twins) do not always develop the same disorders — because their environmental experiences differ. It also has practical implications: even when a diathesis cannot be changed, intervening to reduce stress or build coping resources can reduce the risk of disorder onset.
Limitations include difficulty in operationalising the diathesis concept, since it encompasses genetic, biological, cognitive, and situational factors. The model also focuses on vulnerability rather than resilience — some individuals exposed to both high diathesis and high stress do not develop disorders, and the model provides limited guidance on protective factors that might explain this. More integrative biopsychosocial frameworks have been developed to address these gaps.
Social Learning Theory (covered fully in Unit 1) has specific applications in health psychology, particularly in explaining health-related behaviours and the development of conditions such as substance use, eating disorders, and health behaviour change.
In the context of health, people learn about behaviours such as smoking, dietary practices, exercise habits, and risk-taking through observation of role models — parents, peers, media figures, and cultural figures. If a young person observes that peers who smoke are seen as socially attractive and cool (vicarious reinforcement), they are more likely to adopt the behaviour themselves. Conversely, observing negative health consequences in role models (vicarious punishment) can deter adoption of a behaviour.
Self-efficacy, Bandura's key addition to SLT, is particularly important in health behaviour change. Research consistently shows that individuals with higher self-efficacy for performing healthy behaviours — exercising, stopping smoking, managing diet — are more likely to initiate and maintain those behaviours. Health promotion interventions that focus on building self-efficacy through mastery experiences and role models tend to be more effective than those that rely solely on information or fear appeals.
The social dimension of health behaviour is also captured in the concept of social norms — the shared expectations within a group about what constitutes appropriate behaviour. If unhealthy behaviour (e.g., excessive alcohol consumption) is the perceived norm within a group, social learning processes make it more likely that individual members will adopt it. Conversely, correcting misperceptions about norms can shift behaviour in healthier directions.
Caspi et al. (2003) found that participants with the short allele of the 5-HTT gene who experienced multiple stressful life events were more likely to develop depression. Which model does this finding most directly support?
Answer: B. The diathesis-stress model, because it shows an interaction between genetic vulnerability and environmental stress
Outline the role of two chemical messengers in regulating psychological states and explain why a reductionist account of their role is considered limited.
Command term — "Outline" + "Explain": Give brief, accurate descriptions of two neurotransmitters/hormones (1 mark each) and then provide a reason why reducing psychological states to these chemicals is considered an oversimplification (2 marks).
"Sara grew up in a household where her parents smoked heavily and often joked about smoking-related health warnings. As a teenager, most of her friend group smoked at parties, and nobody seemed to experience negative consequences. By age 19, Sara had taken up smoking regularly. She attempted to quit twice but relapsed both times, telling her GP that she finds it almost impossible to change despite wanting to."
(a) Identify two psychological factors, drawn from Social Learning Theory, that contributed to Sara's uptake of smoking.
(b) Explain how the diathesis-stress model could account for why Sara finds it difficult to quit, even when motivated to do so.
(c) Suggest one SLT-based health intervention that Sara's GP could recommend. Justify your answer.
SL: Discuss the strengths and limitations of the diathesis-stress model in explaining the development of psychological disorders.
HL: "Biological reductionism has advanced our understanding of health and wellbeing, but at the cost of oversimplifying the causes of psychological disorders." Evaluate this claim with reference to relevant research and psychological models.